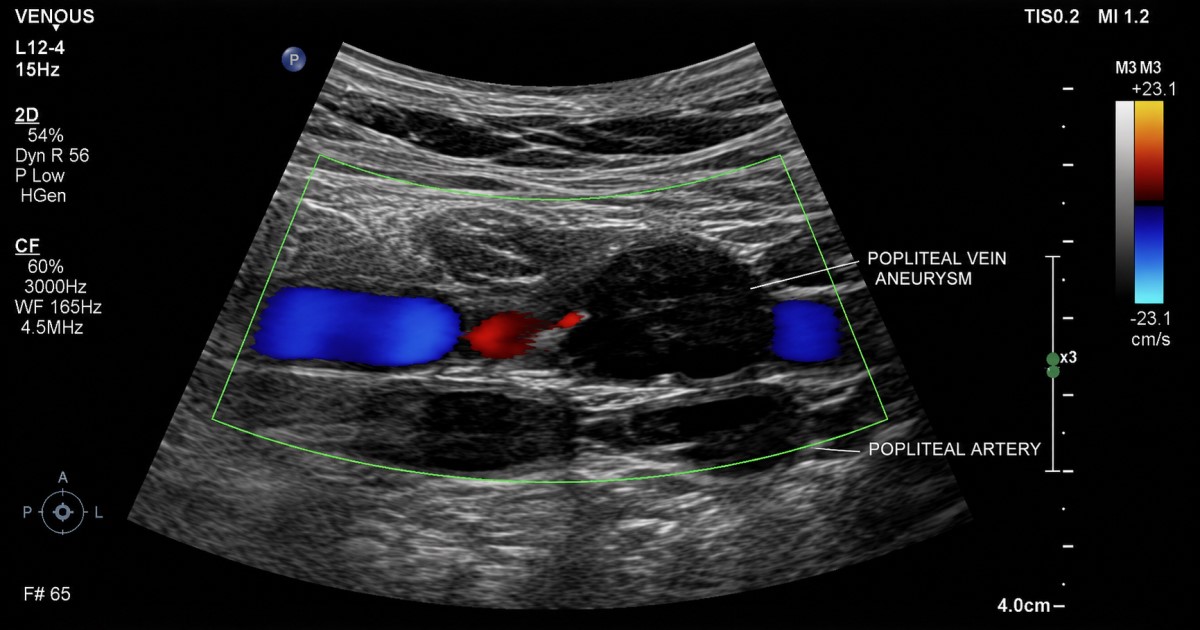

A knee-vein lesion can present in the lungs
Did you know? Pulmonary embolism is reported as the presenting symptom in 70–80% of popliteal venous aneurysm cases.
This makes PVA clinically important far beyond a local finding behind the knee.