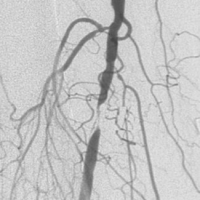
A blocked chest vein can be relieved fast
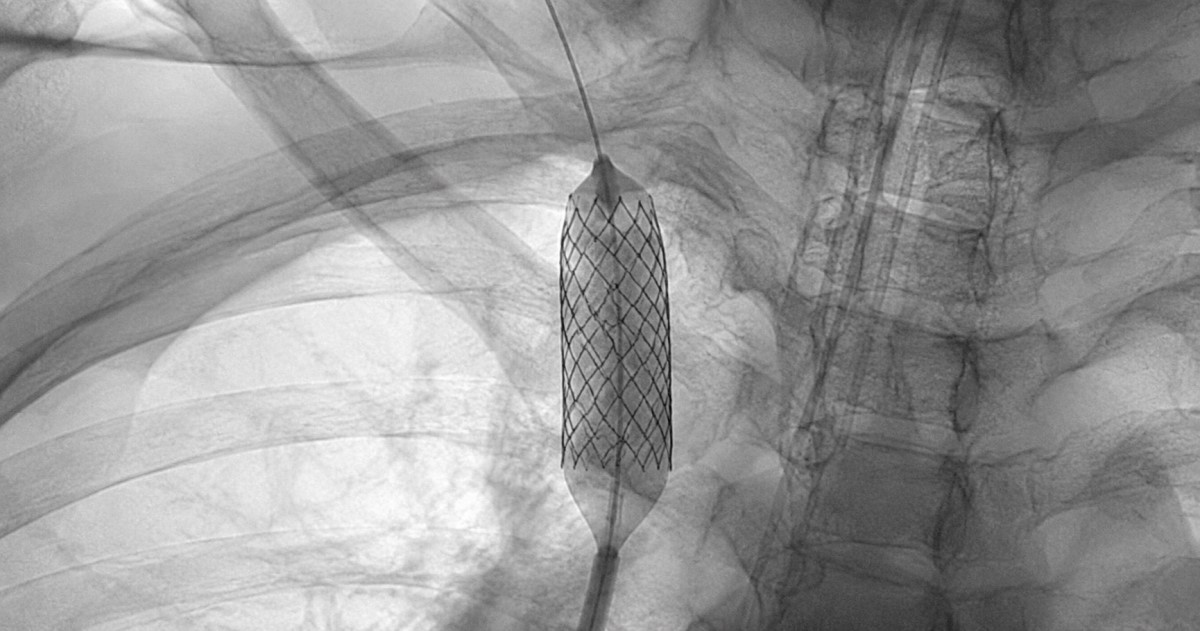
Did you know? In malignant SVCS, stenting reached technical success near 98–99%, symptom relief around 86–94%, and 12-month patency around 80–86%.
This makes SVCS a condition where rapid mechanical palliation may change the immediate clinical pathway.

